
Every year, millions of older adults take more medications than they need. Some of these pills were prescribed years ago for conditions that have since changed-or disappeared. Others were meant to prevent future problems, but now the risks outweigh the benefits. This isn’t just a minor inconvenience. It’s a serious safety issue. Deprescribing isn’t about cutting corners. It’s about removing drugs that no longer serve the person sitting in front of you.
What Exactly Is Deprescribing?
Deprescribing means stopping or lowering the dose of a medicine when the harm it causes is greater than the help it gives. It’s not simply stopping pills. It’s a careful, step-by-step process that looks at the person’s health goals, life expectancy, daily function, and personal preferences. The idea started gaining traction in the early 2000s, when doctors noticed how many seniors were drowning in pills. Today, it’s a recognized part of good geriatric care.Think of it this way: when a doctor prescribes a new drug, they expect it to do something-lower blood pressure, ease pain, prevent a stroke. But when that same drug is renewed every month, no one stops to ask: Is it still doing what it’s supposed to? Deprescribing flips that script. It treats stopping a medication like starting one-something that needs planning, monitoring, and follow-up.
Why Do Seniors End Up With Too Many Medications?
It’s not because doctors are careless. It’s because the system is built for adding, not removing. A senior might see a cardiologist for heart disease, a rheumatologist for arthritis, a neurologist for memory issues, and a primary care doctor for general checkups. Each specialist adds a new medication to treat their specific condition. No one looks at the whole picture.By the time someone turns 75, nearly half of them are taking five or more prescription drugs. In 1994, only 14% of older adults in the U.S. took that many. By 2014, it jumped to 42%. That’s more than triple. And it’s not just quantity-it’s the types of drugs. Some are high-risk: sleeping pills, antipsychotics, painkillers, or long-term proton pump inhibitors (PPIs) for heartburn. These can cause falls, confusion, kidney damage, or even increase the risk of dementia.
When Should Deprescribing Happen?
There are four clear situations where stopping a medication is not just safe-it’s necessary.- New symptoms that might be caused by a drug. If a senior starts having dizziness, confusion, fatigue, or stomach problems after starting a new pill, that pill might be the culprit. Many side effects are mistaken for aging. But they’re often drug reactions. A medication review can untangle this.
- Advanced illness or declining function. If someone has late-stage dementia, is bedbound, or has a life expectancy under a year, some medications make no sense anymore. Preventive drugs like statins for cholesterol or aspirin for heart attack prevention take months or years to show benefit. If the person won’t live long enough to see that benefit, why keep giving them?
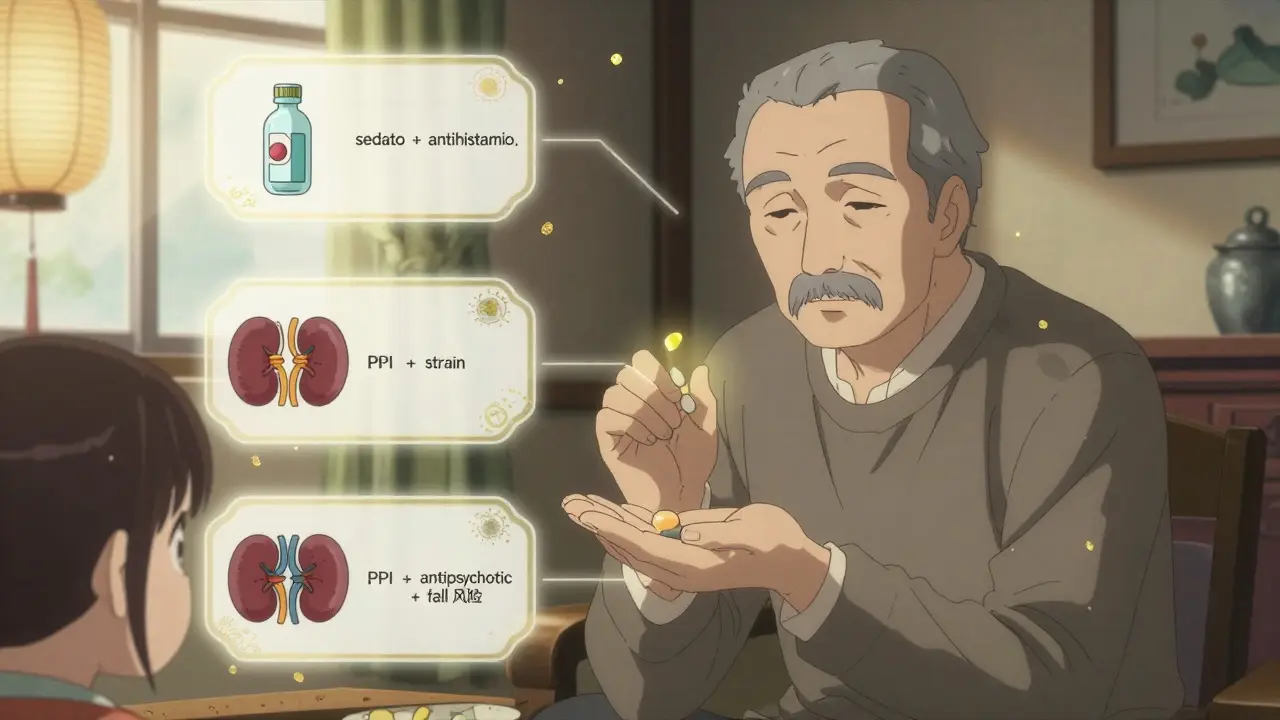
- High-risk drug combinations. Some drugs are dangerous together. For example, mixing a sedative with an antihistamine or a blood thinner with NSAIDs (like ibuprofen) can lead to falls, bleeding, or organ damage. The Beers Criteria and STOPP guidelines list these risky combinations specifically for older adults.
- Preventive drugs with no short-term benefit. Vaccines, bone density meds, or blood pressure pills for someone with no history of heart disease may still be given out of habit. But if the person can’t walk, can’t eat without help, or doesn’t care about living another 10 years, those drugs aren’t helping-they’re just adding pills to the bottle.
How Is Deprescribing Done Right?
You can’t just stop a pill cold turkey. Some medications need to be tapered slowly. Others need monitoring for rebound symptoms. Here’s how it works in practice.- Start with one drug at a time. If you stop three medications at once and the person gets worse, you won’t know which one caused the problem. One at a time lets you see what’s happening.
- Use proven tools. Clinical pharmacists use tools like the Beers Criteria (updated in 2023) and STOPP to identify potentially inappropriate medications. These aren’t just lists-they’re based on years of research.
- Involve the patient. A senior should understand why a drug is being stopped. If they’re scared of withdrawal or think they’ll get sicker, they’ll resist. Clear, simple explanations help. Some clinics even give out short videos or pamphlets explaining why a PPI might be stopped.
- Watch for changes. After stopping a drug, check in within a week or two. Is the person sleeping better? More alert? Less dizzy? Or are symptoms returning? This feedback is critical.
Studies show that when deprescribing is done properly, adverse drug events drop by 17% to 30%. Hospital readmissions fall by 12% to 25%. Quality of life improves-not because the person is healthier, but because they’re not burdened by pills that don’t help.
Who Should Be Involved?
Deprescribing isn’t a one-person job. It takes a team.- Clinical pharmacists are often the best people to lead medication reviews. They’re trained to spot drug interactions, duplicate prescriptions, and outdated treatments. Many hospitals and clinics now have pharmacists dedicated to geriatric care.
- Primary care doctors need to be open to the idea. Too often, they assume specialists know what’s best. But only the primary doctor sees the full picture over time.
- Caregivers and family members play a big role. They’re the ones who notice changes in behavior, appetite, or mobility. They can also help track symptoms after a drug is stopped.
- The senior themselves must be part of the conversation. Their goals matter. Someone who values independence might want to stop a pill that makes them drowsy. Someone focused on comfort might be fine stopping a blood pressure pill that requires daily monitoring.
Common Myths About Stopping Medications
There are a lot of fears around deprescribing. Let’s clear them up.- Myth: “If I stop this, I’ll get worse.” Reality: Many seniors feel better after stopping drugs that cause dizziness, confusion, or fatigue. Stopping a sleeping pill might improve daytime alertness. Stopping an unnecessary painkiller might reduce constipation and improve appetite.
- Myth: “My doctor wouldn’t prescribe it if it wasn’t needed.” Reality: Prescriptions often continue out of habit. A drug prescribed for a past condition might not be relevant anymore. That’s why reviews are needed.
- Myth: “All medications are safe if taken as directed.” Reality: No drug is risk-free, especially in older adults. Their bodies process medicine differently. What’s safe at 50 might be dangerous at 80.
What If You’re Not Sure?
If you’re worried about a medication your senior loved one is taking, don’t wait. Ask for a full medication review. You can request this from their primary care doctor, pharmacist, or even a geriatric specialist. Many community pharmacies now offer free medication reviews for seniors.Bring all the pills in a bag-prescription, over-the-counter, vitamins, herbal supplements. The pharmacist or doctor will go through them one by one. They’ll check for duplicates, outdated uses, dangerous interactions, and whether the drug still matches the person’s current health goals.
And remember: if a medication was started as a trial, it should be reviewed as a trial. If it’s been refilled for years without a check-in, that’s a red flag.
What’s Next for Deprescribing?
The future of deprescribing is getting smarter. Electronic health records are now being programmed to flag high-risk prescriptions for seniors. Some clinics use AI tools that analyze a patient’s history and suggest which drugs might be safe to stop. Mobile apps like those from Deprescribing.org give patients step-by-step guides to talk to their doctors.More importantly, guidelines are shifting. The World Health Organization now lists deprescribing as a key part of global patient safety. Medicare and Medicaid are starting to track deprescribing rates as a quality measure. This isn’t just a trend-it’s becoming standard care.
For seniors, the goal isn’t to take fewer pills just for the sake of it. It’s to take only the ones that help them live better-more alert, more mobile, more in control of their own lives.
Can stopping medications make someone sicker?
Sometimes, yes-but only if done incorrectly. Stopping certain drugs suddenly, like blood pressure medications or antidepressants, can cause withdrawal effects. That’s why deprescribing is never random. It’s planned, gradual, and monitored. The goal is to remove drugs that are more likely to harm than help, not to stop everything. When done right, most seniors feel better, not worse.
Is deprescribing only for people in nursing homes?
No. In fact, most older adults live at home, not in care facilities. That’s why deprescribing is so important in community settings. People managing their own meds with help from family are at higher risk of taking unnecessary or dangerous drugs. Home-based medication reviews by pharmacists have been shown to reduce inappropriate prescribing just as effectively as hospital-based ones.
Do I need to see a specialist to start deprescribing?
Not at all. Your primary care doctor or pharmacist can start the process. Many community pharmacies offer free medication reviews for seniors. You don’t need a referral. Just bring your pill bottle or list of medications to your next appointment and ask: "Could any of these be stopped or lowered?"
What if my doctor says a drug is "just in case"?
"Just in case" is not a medical reason to keep a drug. Preventive medications only help if the person lives long enough to benefit. For someone with limited life expectancy or severe frailty, "just in case" drugs often do more harm than good. Ask your doctor: "What specific problem is this drug preventing? How likely is that problem? And how long will it take to see a benefit?" If the answer is "we don’t know" or "it might help in 5 years," it’s worth reconsidering.
Are there any medications that should never be stopped?
No medication is automatically off-limits. Even essential drugs like insulin, heart medications, or seizure control drugs can be reconsidered if the person’s condition has changed. For example, if someone with diabetes becomes severely frail and can’t eat regularly, lowering insulin might prevent dangerous lows. The key is individualization-not blanket rules. Every drug should be reviewed in the context of the person’s current health, goals, and risks.



Too many seniors are just handed pills like candy and told to take 'em every day. No one ever asks if they still need 'em. I saw my uncle go from alert and sharp to a zombie just from stacking 8 meds. One review, 3 stopped, and he started cooking again. Simple as that.
Yessssss. This is the kind of thing we need more of. My grandma’s on a beta-blocker she hasn’t needed since 2017. She’s 89, walks with a cane, and hates that she can’t nap in the afternoon. We asked. They tapered it. Now she’s napping on her own terms. 🙌
I’m a geriatric nurse and I see this daily. The scariest part? People think stopping meds = giving up. But it’s the opposite. It’s reclaiming life. One woman I worked with was on 11 meds. After deprescribing, she went back to gardening. Said she finally felt like herself again. 💛
Let’s be honest-the pharmaceutical-industrial complex thrives on perpetual prescription cycles. Deprescribing is not just medical-it’s ideological. It challenges the very notion that intervention equals care. We’ve pathologized aging, and now we medicate it into submission. The real question isn’t whether to stop drugs-it’s why we ever started them in the first place.
Wait wait wait. You’re telling me we’re supposed to just stop meds because someone’s 'not living long enough' to benefit? What if they live longer than expected? What if the doctor didn’t know? What if the system is rigged by Big Pharma to keep people on drugs? I’ve seen people get worse after stopping. I’ve seen people die. Who’s accountable? Who signed off? You can’t just flip a switch on insulin or anticoagulants. This is dangerous. And they’re pushing this as 'standard care'? I don’t trust this.
I’ve been quietly reviewing my dad’s meds for a year. He’s 82, has mild COPD, and takes 7 prescriptions. I brought them all to his pharmacist-no referral needed. They found two duplicates, one that was for a condition he’d outgrown, and a PPI he’d been on since 2010. Stopped them one by one. He’s sleeping better, eating more, and hasn’t fallen once since. No drama. No crisis. Just common sense. I wish more families did this. It’s not hard. Just ask.
Oh honey, I love how you’re all so sweet about deprescribing. But let’s be real-most of these seniors don’t even know what’s in their own medicine cabinet. I had a client who was taking four different painkillers, all for 'arthritis,' but she couldn’t even tell me what they were. And now you want her to 'decide' if she should stop them? Sweetie, she needs someone to hold her hand and say, 'This one? We’re done.' Not a conversation. A rescue.
It’s not about fewer pills. It’s about better living. One drug. One goal. One life. That’s the equation. Everything else is noise.