Stopping a high-dose steroid cold turkey isn't just a bad idea-it can be life-threatening. When you take medications like prednisone for more than a few weeks, your body essentially goes on vacation from producing its own cortisol. If you suddenly cut off the external supply, your adrenal glands might not wake up fast enough, leading to a dangerous drop in blood pressure and organ failure. This is why steroid tapering is a non-negotiable part of treatment for autoimmune diseases.
The goal is to trick your body into starting its own production again while keeping your original illness under wraps. It's a delicate balancing act: go too fast, and you hit a wall of withdrawal; go too slow, and you deal with side effects longer than necessary. Whether you're managing rheumatoid arthritis or a severe allergic reaction, knowing how the process works can take the anxiety out of the wind-down.
Why You Can't Just Stop Taking Steroids
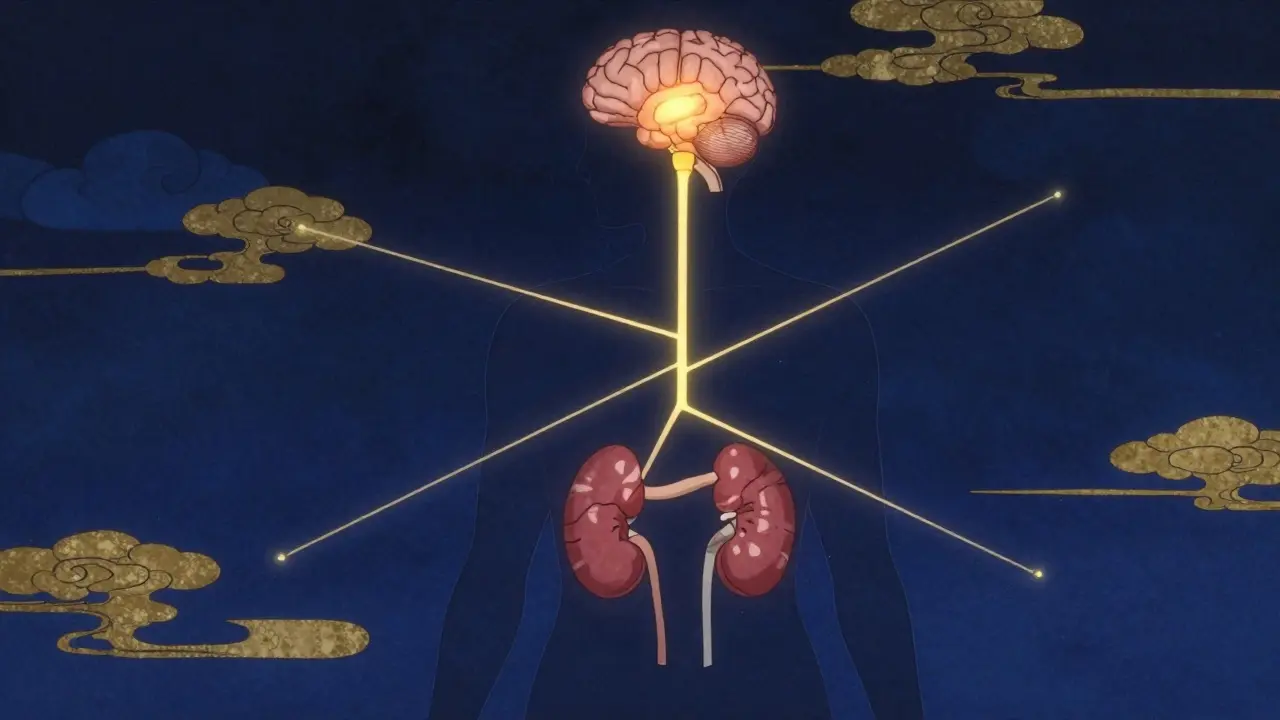
To understand the danger, you have to understand the HPA axis. This is the communication line between your hypothalamus, pituitary gland, and adrenal glands. Normally, they work together to release cortisol, the body's natural stress hormone. However, Glucocorticoids-the class of synthetic steroids used to fight inflammation-mimic cortisol so well that your brain thinks it has plenty. As a result, it tells your adrenal glands to stop working.
If you stop the medication abruptly, you enter a state of Adrenal Insufficiency. Because your natural cortisol production is dormant, your body can't handle basic stress. A simple flu or a stressful day at work could trigger an adrenal crisis, characterized by severe hypotension (low blood pressure) and shock. This is why doctors use a tapering schedule to slowly "wake up" the HPA axis.
The Tapering Process: What to Expect
Tapering isn't a one-size-fits-all plan. A person who took steroids for ten days needs a very different approach than someone who has been on them for two years. Generally, the process is broken into three phases based on the dose of Prednisone or its equivalent.
In the initial phase, if you're on a high dose (above 20-40 mg), the reductions are often larger. You might drop 5-10 mg every week. It feels fast, but the body is more resilient at these higher levels. Once you hit the 20 mg mark, things slow down. This is where the "gradual taper" kicks in, often reducing by 2.5 mg or 5 mg every couple of weeks.
The final stretch-dropping below 10 mg-is often the hardest. This is where many people experience "taper tantrums." Even a tiny drop from 5 mg to 2.5 mg can feel like a huge jump because the dose is now closer to what your body would naturally produce. For some, this final phase can take several weeks or even months to ensure the adrenal glands have fully resumed control.
| Phase | Dose Range | Typical Reduction Rate | Primary Focus |
|---|---|---|---|
| Initial Rapid | > 20-40 mg/day | 5-10 mg weekly | Reducing systemic load |
| Gradual | 10-20 mg/day | 2.5-5 mg every 1-2 weeks | Monitoring for withdrawal |
| Slow/Final | < 10 mg/day | 1.25-2.5 mg every 2 weeks | HPA axis recovery |

Dealing with Withdrawal and Disease Rebound
There is a big difference between Glucocorticoid Withdrawal Syndrome (GWS) and a disease flare. GWS feels like a general "flu-like" state: joint pain, muscle aches, extreme fatigue, and sometimes mood swings or insomnia. It's not that your autoimmune disease is back; it's that your body is craving the drug.
A disease rebound, however, is when the original condition-like Rheumatoid Arthritis or Inflammatory Bowel Disease-returns because the medication is no longer strong enough to suppress it. If you notice the specific symptoms you had before starting steroids (like a swollen joint or digestive distress), that's a rebound, not withdrawal.
To manage these, some doctors suggest switching to Hydrocortisone during the final stages. Because it has a shorter half-life and more closely resembles natural cortisol, it can sometimes make the transition easier, though many patients successfully taper off prednisolone directly.

Practical Tips for a Smoother Transition
Tapering is as much a mental game as a physical one. Being proactive can significantly lower the intensity of the side effects. Here are a few strategies based on patient outcomes:
- Keep a Symptom Log: Track your mood, energy, and pain levels daily. This helps your doctor decide if you need to hold at a certain dose for an extra week before dropping again.
- Gentle Movement: Don't jump into a HIIT workout, but don't stay in bed. Short, 15-minute walks twice a day can reduce the muscle stiffness associated with withdrawal by over 50%.
- Mindset and Stress Management: Cortisol is the stress hormone. When your levels are fluctuating, you might feel more anxious. 10 minutes of daily meditation or deep breathing can noticeably lower the perceived severity of withdrawal.
- The "Sick Day" Rule: If you get a high fever or a severe infection while tapering, your body needs more cortisol than usual. Talk to your doctor about "stress dosing"-temporarily increasing your dose during acute illness to prevent a crash.
One of the most overlooked tools is the steroid alert card. If you've been on long-term therapy, your HPA axis might take up to 18 months to fully recover. Carrying a card that notifies emergency responders that you've recently been on steroids can be a lifesaver if you're unconscious during an accident.
When to Call Your Doctor Immediately
While some fatigue is normal, certain signs mean the taper is going too fast or you're in danger. You should seek medical help if you experience:
- Severe Dizziness or Fainting: This can be a sign of hypotension, indicating your body isn't producing enough cortisol.
- Nausea and Vomiting: Sudden gastrointestinal distress combined with weakness is a red flag for adrenal crisis.
- Rapid Return of Primary Symptoms: If your autoimmune disease flares up violently, you may need a slower taper or a different maintenance medication.
- Mental Confusion: Severe "brain fog" or disorientation beyond typical fatigue needs immediate attention.
How long does a steroid taper usually take?
It depends entirely on how long you were taking the meds. If you used them for under three weeks, a 1-2 week taper might suffice. For those on long-term therapy (6 months or more), the process can take 3 to 6 months to ensure the adrenal glands safely restart.
Can I use a supplement to help with steroid withdrawal?
Always consult your doctor first. While some people look into adrenal support supplements, they can interfere with the very process of waking up your HPA axis. Focus on anti-inflammatory nutrition and gentle exercise instead.
What is the difference between a flare and withdrawal?
Withdrawal (GWS) is a systemic response-general fatigue, muscle aches, and moodiness. A flare is a return of your specific disease symptoms, such as joint swelling in arthritis or skin rashes in lupus.
Why do some doctors switch me to hydrocortisone?
Hydrocortisone has a shorter biological half-life than prednisolone. This means it leaves the system faster, which some clinicians believe encourages the body's natural cortisol production to kick back in more efficiently.
Is it possible to fail a taper and have to go back on steroids?
Yes. If a disease rebound occurs, you may need to increase the dose again. This doesn't mean the treatment failed; it just means the disease activity is still too high. In these cases, doctors may switch to a "disease activity-guided taper" rather than a fixed schedule.


The mention of the steroid alert card is a huge point here. A lot of people forget that the HPA axis doesn't just snap back the second you hit zero mg. I've seen folks think they're in the clear and then they have a minor car accident or a bad flu and suddenly they're in an adrenal crisis because the EMTs didn't know their history. Definitely keep that card in your wallet or set up a medical ID on your phone lock screen if you've been on these for months.
It is truly fascinating how the average individual underestimates the biochemical complexity of the endocrine system. Most people simply view medication as a binary switch-on or off-failing to comprehend that the human body is a symphony of feedback loops. The HPA axis is not merely a communication line; it is a delicate homeostasis that, once disrupted by exogenous glucocorticoids, requires an almost ritualistic patience to restore. To rush this process is to invite biological chaos, a lesson in humility that many only learn after experiencing the precipice of organ failure.
Oh great, just what I needed-the reminder that my body is basically a lazy teenager who refuses to wake up and do its job once it gets a little bit of help from a pill. Truly a miracle of evolution.
I went through this last year and it was an absolute NIGHTMARE! I felt like my entire soul was leaving my body during the final 5mg drop! One day I'm fine, the next I'm weeping on the kitchen floor because I can't open a jar of pickles! It is the most harrowing experience a human being can endure without actually being in a war zone! Total devastation!
I really appreciate how this explains the difference between a flare and withdrawal because it can be so confusing when you're in the middle of it and you don't know if you're getting sick again or if your body is just reacting to the change in medication, but if you just take it one day at a time and keep that symptom log mentioned above, you'll find that the mental burden becomes much lighter and you can actually start to see the progress you're making toward health.
Omg right?? The 'taper tantrums' are so real!!! 🙄 I literally felt like a toddler again just because of some meds!!! Absolute madness!!!! 💅✨
too long.
You all have to keep pushing through the fatigue because the feeling of finally being off the medication is the most rewarding victory you can achieve for your long-term health and wellness! Even when the joint pain hits or the brain fog makes you feel like you're walking through mud, just remember that every single milligram you drop is a step closer to regaining your natural strength and you are much stronger than a little bit of withdrawal symptoms so stay focused and keep moving forward with everything you've got!