Most people think of melanoma when they hear "skin cancer." But the truth is, two other types - basal cell carcinoma and squamous cell carcinoma - are far more common. Together, they make up about 95% of all nonmelanoma skin cancers. If you’ve noticed a weird bump, sore that won’t heal, or scaly patch on your skin, it’s worth knowing the difference between these two. One grows slowly and rarely spreads. The other can move fast and, in rare cases, become life-threatening. Understanding the difference isn’t just about labels - it’s about catching it early, treating it right, and knowing what to watch for next.
Where They Start: The Skin’s Layers
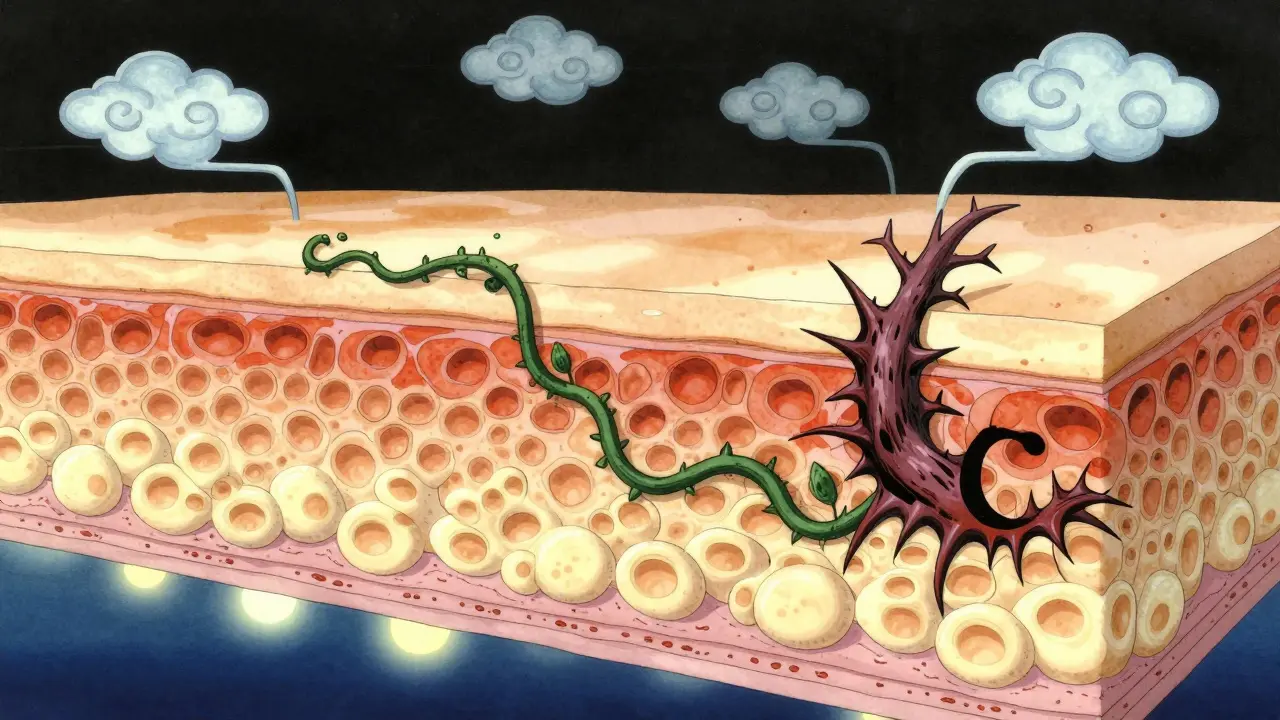
Your skin isn’t just one layer. It’s stacked like a cake. At the very bottom is the basal layer, where new skin cells are born. These cells slowly push upward, flatten out, and become squamous cells by the time they reach the surface. Basal cell carcinoma starts in that bottom layer. Squamous cell carcinoma starts higher up, in the flattened cells near the top. That tiny difference in origin changes everything - how they look, how they act, and how dangerous they can be.
What They Look Like: Spotting the Signs
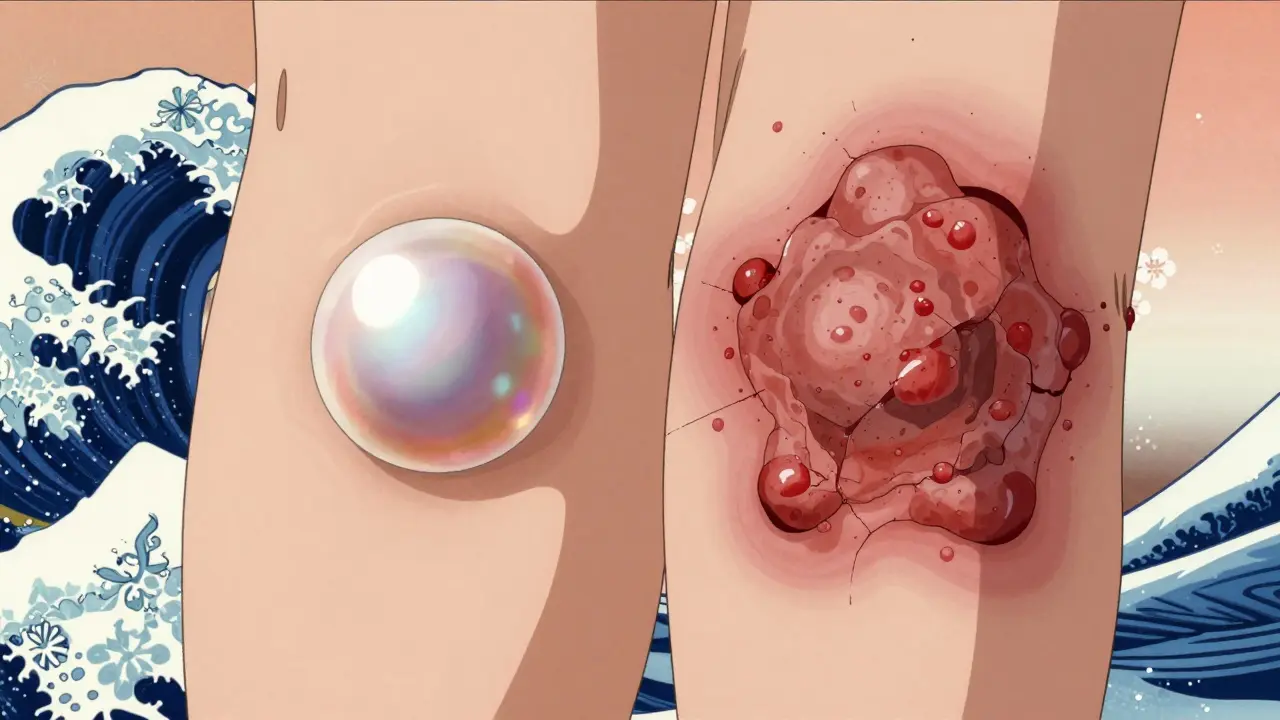
Basal cell carcinoma (BCC) often shows up as a shiny, pearly bump - kind of like a tiny pearl under the skin. Sometimes it’s a flat, waxy patch that looks like a scar. Or it might be an open sore that bleeds, crusts over, and never fully closes. You’ll usually find it on your face, ears, or neck - places hit hardest by the sun. About 70% of BCCs are pearly bumps. The rest are sores or scars.
Squamous cell carcinoma (SCC) looks different. It’s often a firm, red bump, like a wart. Or it could be a rough, scaly patch that flares up and doesn’t go away. It might bleed easily or crust over. SCC can also show up as an ulcer - a deep sore that doesn’t heal. It’s more likely than BCC to appear on your lips, ears, hands, or scalp. And unlike BCC, SCC can grow quickly. Some lesions double in size within weeks.
How Fast They Grow: Speed Matters
BCC creeps along. On average, it grows about half a centimeter to one centimeter per year. That’s why many people ignore it for months - or even years. But don’t be fooled. Even slow growth can destroy tissue. Left untreated, 70% of advanced BCCs invade deeper layers of skin, cartilage, or bone.
SCC moves faster. It grows about 1.5 to 2 centimeters per year - three times quicker than BCC. Aggressive forms can balloon in size within a month. That’s why doctors warn: if a spot changes fast, don’t wait. A lesion that grows noticeably over 4-6 weeks needs evaluation. Speed is a red flag.
How Dangerous They Are: The Metastasis Risk
This is where the big difference lies. BCC almost never spreads. Less than 0.1% of cases metastasize. Even when it’s large or neglected, it stays local. It’s more of a "destroy your nose" problem than a "spread to your lungs" problem.
SCC is different. While most cases are caught early and cured, 2-5% of SCCs spread to lymph nodes or other organs. That number jumps to 14% if it’s on the lip, 9% on the ear, or 7% on the genitals. Once it spreads, survival drops from 95% to 25-45%. That’s why SCC is the second leading cause of skin cancer deaths after melanoma.
Who Gets It: Risk Factors
Both cancers are tied to sun exposure. But not in the same way. BCC often links to intense, occasional sunburns - think weekend beach trips or childhood tans. SCC is more about lifelong, cumulative exposure. That’s why outdoor workers, farmers, and people in high-sun regions like Australia have higher rates.
Age matters too. 85% of cases happen after age 50. The average diagnosis age is 67 for both, but SCC is slightly older - 69 on average. Fair skin, light eyes, and a history of sunburns increase risk. Men are more likely to get SCC - 65% of cases - probably because of longer occupational sun exposure. BCC affects men and women more evenly.
Immunosuppressed people - like organ transplant recipients - face a 250-fold higher risk of SCC and a 10-fold higher risk of BCC. That’s a huge gap. It shows SCC is more sensitive to immune system weakness.
Treatment: What Works and What Doesn’t
Both cancers respond well to treatment - if caught early. Surgical removal cures 95-98% of primary cases. Mohs surgery, where layers are removed and checked under a microscope until no cancer remains, gives the highest cure rates: 99% for BCC, 97% for SCC.
But treatment isn’t the same for both. BCC can sometimes be treated with topical creams like imiquimod or 5-fluorouracil - especially for superficial types. These work in 60-70% of cases. For SCC? Only 40-50% effective. That’s why doctors rarely rely on creams alone for SCC.
SCC needs wider surgical margins - 4-10 millimeters - because it tends to spread deeper under the skin. BCC usually needs only 3-5 mm. That means more tissue removed, more scarring, and often more reconstructive surgery for SCC patients. In fact, 45% of SCC cases need reconstruction versus 28% for BCC.
For advanced cases, immunotherapy is changing the game. Cemiplimab (Libtayo) is FDA-approved for metastatic SCC and works in nearly half of patients. No such drug exists yet for advanced BCC - instead, hedgehog inhibitors like vismodegib are used. They’re effective but come with serious side effects.
Recovery and Follow-Up
Most BCC patients get cured with one treatment. 92% achieve complete clearance after a single session. SCC patients? Only 78%. They need more follow-ups - on average, 2.3 times more visits than BCC patients. Why? Because SCC has a higher chance of coming back. In high-risk patients, 73% of recurrent SCCs show up within a year. BCC recurrences take longer - often 18 months or more.
Patients report more anxiety with SCC. On forums like Reddit, 85% of SCC patients worry about metastasis. Only 42% of BCC patients do. That fear isn’t irrational. It’s based on real risk. And it’s why doctors stress vigilance after SCC treatment.

Prevention: Sun Protection Works - But Differently
Daily sunscreen cuts BCC risk by 40%. For SCC? It cuts it by 50%. That’s because SCC is more directly tied to long-term UV damage. Sunscreen helps both, but it’s even more critical for preventing SCC.
Wear a hat. Seek shade. Avoid midday sun. Don’t use tanning beds. These aren’t just good ideas - they’re proven shields. Australia, with its high UV levels, has one of the highest SCC rates in the world. Public health campaigns there have cut skin cancer deaths - but not fast enough. Prevention still beats treatment every time.
What Comes Next: New Tools and Hope
Science is catching up. AI tools are now being trained to tell BCC and SCC apart using dermoscopy images. Early results show 94% accuracy - better than many dermatologists. That means faster, more accurate diagnoses.
Researchers are also finding genetic markers that predict which SCCs are likely to spread. Twelve genes have been linked to high metastasis risk. In the future, a simple biopsy might tell you not just "what it is," but "how dangerous it is." That’s personalizing treatment before it even begins.
Photodynamic therapy - using light and drugs to kill cancer cells - is improving too. It clears 92% of superficial SCCs and 85% of BCCs. It’s less invasive than surgery and leaves less scarring. For older patients or those with multiple lesions, it’s becoming a real option.
Bottom Line: Know the Difference, Act Fast
Basal cell carcinoma is the most common cancer in humans. But it’s rarely deadly. Squamous cell carcinoma is less common - but more dangerous. One is a slow, stubborn intruder. The other can turn into a fast-moving threat. Neither should be ignored. If you see a spot that won’t heal, bleeds easily, grows quickly, or changes shape - get it checked. Early detection means simple treatment. Delayed care means bigger surgery, more scans, and higher risk.
Don’t wait for a doctor to find it. Look at your skin every month. Check your face, neck, ears, hands - anywhere sun hits. Take a photo if you need to track changes. And if you’ve had one skin cancer, you’re at higher risk for another. Quarterly skin checks aren’t optional - they’re essential.
Both cancers are preventable. Both are treatable. But only if you know what to look for - and act before it’s too late.
Can basal cell carcinoma turn into squamous cell carcinoma?
No, basal cell carcinoma cannot turn into squamous cell carcinoma. They start from different cells in the skin and are separate diseases. Having one doesn’t mean you’ll get the other - but having one skin cancer increases your overall risk of developing another type, including SCC or even melanoma. That’s why regular skin checks are so important.
Is squamous cell carcinoma more serious than basal cell carcinoma?
Yes, in terms of potential danger. While BCC is far more common, SCC has a higher risk of spreading to other parts of the body. Even though most SCCs are cured when caught early, about 2-5% metastasize - compared to less than 0.1% for BCC. When SCC spreads, survival rates drop sharply. That’s why doctors treat SCC more aggressively, especially if it’s on the lips, ears, or in immunocompromised patients.
How do I know if a skin spot is cancerous?
Look for the ABCDEs of skin cancer - but adapted for nonmelanoma types. For BCC: a shiny, pearly bump or a sore that bleeds and doesn’t heal. For SCC: a firm red bump, scaly patch, or ulcer that grows fast. Any new, changing, or non-healing spot after two weeks deserves a dermatologist’s eye. Don’t rely on self-diagnosis. A biopsy is the only way to know for sure.
Can I treat basal or squamous cell carcinoma at home?
Only under a doctor’s supervision. Topical creams like imiquimod or 5-fluorouracil can treat some superficial BCCs, but they’re not reliable for SCC. Over-the-counter remedies, essential oils, or home remedies won’t cure skin cancer. Delaying proper treatment allows the cancer to grow deeper - making surgery harder and increasing risk of spread. Always see a dermatologist first.
How often should I get my skin checked after treatment?
If you’ve had BCC, annual skin checks are usually enough. But if you’ve had SCC - especially if it was high-risk - you need checks every 3-6 months for at least two years. Recurrence is most likely in the first year. After that, yearly checks are still recommended. People with a history of skin cancer are at higher risk for new ones. Vigilance saves lives.
Does sunscreen prevent both types of skin cancer?
Yes - and it works better for squamous cell carcinoma. Daily sunscreen use reduces SCC risk by 50% and BCC risk by 40%. That’s because SCC is more directly linked to long-term sun exposure, while BCC is often tied to intense, intermittent burns. Still, sunscreen is your best defense against both. Use broad-spectrum SPF 30+, reapply every two hours, and don’t forget your ears, lips, and hands.




i legit thought bcc was just a weird pimple that never went away. never knew it could grow into your nose bone. thanks for the heads up. i’m gonna start checking my face like it’s a crime scene now. also typo: i meant ‘creepy’ not ‘creep’ but you get it lol
so if it grows slow it’s bad but if it grows fast it’s worse? i’m confused. is it like a slow burn fire or a bomb? also why do they call it ‘squamous’? sounds like a dinosaur name.
Let me tell you something. The medical industry is milking this. They want you scared. They want you coming back every 3 months. They want you spending $2,000 on Mohs surgery when a little tea tree oil would’ve done the trick. I know people. I know what’s really going on. And they’re not telling you the truth about immunotherapy. It’s just a cover for Big Pharma’s next cash grab.
And don’t get me started on sunscreen. That stuff’s full of endocrine disruptors. You’re trading one cancer for another. The sun is your friend. Your ancestors didn’t wear SPF 50 and they lived to 90.
There’s something poetic about how the skin remembers every hour spent under the sun. Each bump, each patch - they’re not just cells gone wrong. They’re stories. The farmer’s ear, the child’s summer burn, the office worker who finally took a vacation. We think of cancer as an enemy, but maybe it’s just the body’s way of screaming, ‘I’ve been ignored too long.’
And yet, we still treat it like a mistake to fix, not a warning to hear. Maybe the real cure isn’t in the scalpel or the cream, but in learning to live gently with the earth we’re given.
My uncle had SCC on his lip. He didn’t go to the doctor until it bled when he ate. He said, ‘It’s just a sore.’ He’s gone now. I don’t blame him. I blame the silence.
So when you look at your skin, don’t just look for spots. Look for time. Look for your own history. And if you see something that won’t heal? Don’t wait. Don’t rationalize. Just go. For yourself. For the ones who didn’t.
As someone who grew up in Jakarta but now lives in Arizona, I’ve seen how sun exposure hits different depending on where you are. Back home, we wore sarongs and hats to block the sun - not because we were scared of cancer, but because it was just what you did. Here, people burn like marshmallows and then blame the ‘bad ozone.’
Also, I love that AI can now tell BCC from SCC. But I wonder - will that tech be available in rural India or Nigeria? Or will it just help rich folks in Texas get faster diagnoses? We need to make this knowledge global, not just convenient.
And hey - sunscreen isn’t just for beach days. I put it on my neck every morning before work. No shame. My mom’s from Kerala and she still says, ‘Sun is not your friend, beta.’ She was right.
So let me get this straight - BCC is the boring cousin who never leaves the house but slowly eats your face, and SCC is the party animal who shows up drunk, starts a fight, and then vanishes to another country? Yeah, that’s basically the vibe.
Also, 85% of SCC patients worry about metastasis? Bro. I’d be checking my lymph nodes every 10 minutes too. I’d probably Google ‘is my ear swollen cancer’ at 3 a.m. and then cry. Thanks for that, article.
And yes, I just used ‘bro.’ I’m trying to be casual. I’m not a robot. Mostly.
Did you know the WHO says 90% of skin cancers are preventable? That means anyone who gets this is basically choosing to be reckless. No one’s forcing you to tan. No one’s forcing you to skip sunscreen. This isn’t bad luck - it’s poor life choices. If you don’t protect yourself, don’t cry when the bill comes. America is the land of freedom - and consequences.
My dad had BCC on his ear and they cut it out with a scalpel and he didn’t even need stitches. It was fine. But now I’m paranoid about every mole. I’ve been checking my skin every day. I think I have three SCCs already. I’m going to the dermatologist tomorrow. I just hope they don’t charge me for the anxiety.
My cousin in Delhi got SCC on his scalp from working under the sun for 30 years. He didn’t know it was cancer until he lost hair in a patch. Now he wears a cap always. But here’s the thing - he didn’t have money for Mohs. They used cryotherapy. It worked. So don’t think you need fancy surgery. Just get it checked. Early. No matter where you are.
Also - sunscreen in India? Most people think it’s for rich people. But I bought a ₹150 tube last year. I use it every day. It’s not about money. It’s about respect for your body.