
Vitamin K Intake Tracker
Track Your Vitamin K Intake
Your goal is to consume 60-120 µg of vitamin K daily. Consistency matters more than the exact amount.
Add Vitamin K Sources
Daily Tracking
Track Your Consistency
Consistency is key to stable INR levels. Record your intake for 4-6 weeks to find your personal rhythm.
Pro Tip: Eat the same amount of vitamin K-rich foods on the same days each week. For example, 1 cup of raw kale every Tuesday and Thursday.
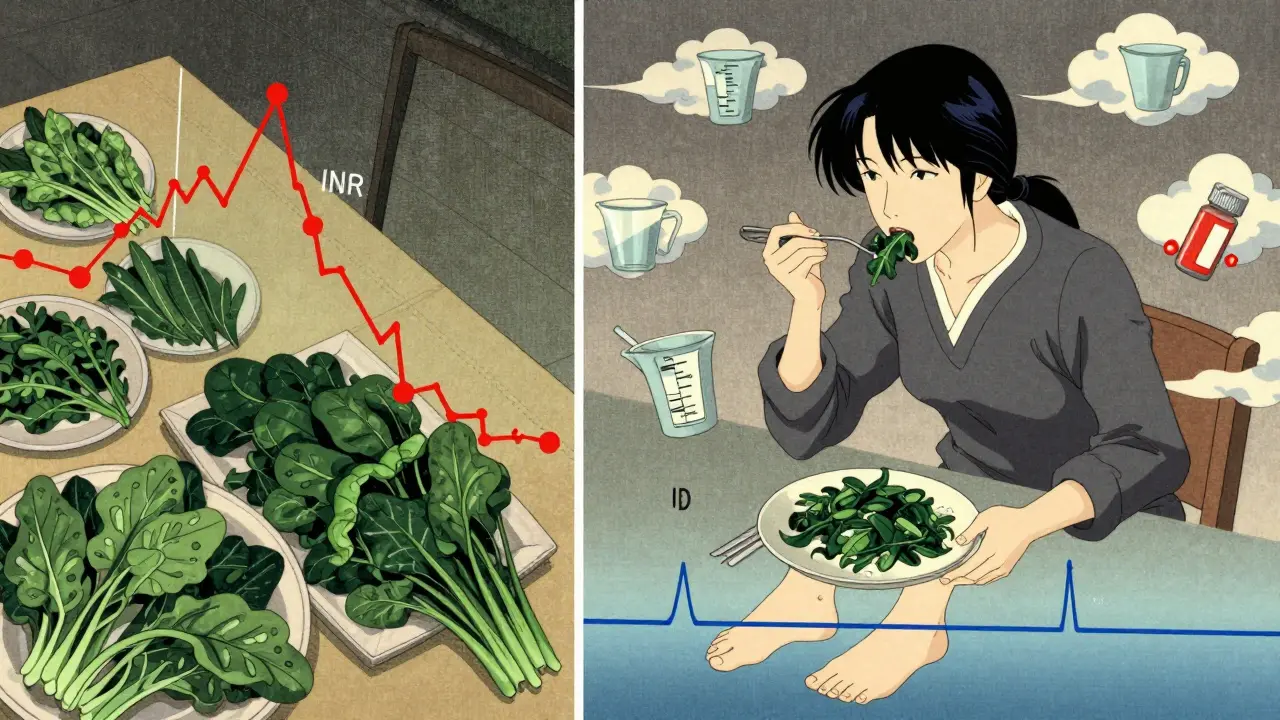
When you're on warfarin, your life doesn't change because of the drug - it changes because of what you eat. Not because you have to avoid greens, but because consistency is the only thing that keeps your INR stable. Too much vitamin K one day, too little the next, and your blood either clots when it shouldn't or bleeds when it should stay still. This isn't about restriction. It's about rhythm.
Why Warfarin and Vitamin K Are Locked in a Chemical Dance
Warfarin works by blocking a single enzyme: VKORC1. That enzyme’s job is to recycle vitamin K so your body can make clotting factors - proteins that stop you from bleeding out after an injury. Without enough active vitamin K, those proteins don’t form properly. That’s the point. You want your blood to thin just enough to prevent clots from forming in your heart or legs, but not so much that a bump turns into a bruise the size of a dinner plate.
Vitamin K, mostly from leafy greens like spinach, kale, and broccoli, is the exact opposite of what warfarin wants. It’s the fuel your body needs to rebuild those clotting factors. So if you eat a big bowl of kale on Monday and nothing green all week, your body gets a surge of vitamin K, then a drought. That swing throws your INR off - sometimes dangerously so.
Studies show patients with inconsistent vitamin K intake have 2.3 times more INR fluctuations than those who eat about the same amount every day. That’s not a small risk. It means more doctor visits, more blood tests, and a higher chance of a stroke or internal bleed.
The Myth of ‘Avoid Greens’ - And Why It’s Dangerous
For years, doctors told patients on warfarin to stay away from vitamin K-rich foods. The logic seemed simple: less K = more predictable blood thinning. But here’s the truth: restricting vitamin K actually makes INR control worse.
A 2021 guideline from the American College of Chest Physicians flipped the script. They now say: “Dietary vitamin K restriction is not recommended and may be harmful.” Why? Because when you cut out greens, your body starts to run low on vitamin K. That makes your clotting factors under-carboxylated - meaning they don’t work right even when you finally eat them. The result? Wild INR swings.
One study found patients who avoided vitamin K had 37% more day-to-day INR variability than those who ate it regularly. That’s not safer. That’s riskier. Your body needs a steady trickle of vitamin K to stay balanced. Starving it doesn’t help - it confuses it.
What’s the Right Amount? Not What You Think
The Recommended Dietary Allowance (RDA) for vitamin K is 90 µg/day for women and 120 µg/day for men. Sounds simple, right? But here’s the twist: most people in the U.S. already eat close to that. The average woman eats 93 µg, the average man 122 µg. So you’re not likely deficient. You’re likely inconsistent.
The goal isn’t to hit the RDA. It’s to stay within a narrow range - 60 to 120 µg per day, consistently. That’s about one cup of cooked spinach (889 µg) or one cup of raw kale (547 µg) spread out over several meals during the week. Not all at once. Not once a month.
Think of it like this: if you usually eat 100 µg of vitamin K on Tuesday and Thursday, keep doing that. If you suddenly swap your spinach salad for a carrot stick, your INR might spike. If you go from no greens for a week to a giant kale smoothie, your INR might crash. Both are dangerous.
Real-Life Examples: How People Got It Right
One Reddit user, u/WarfarinWarrior, shared how their INR went from all over the place to rock solid. Their pharmacist gave them a simple tracker: “Eat exactly one cup of mixed greens every Tuesday and Thursday.” No more guessing. No more fear. Just routine. Their time in therapeutic range (TTR) jumped from 45% to 78% in two months.
Another example: a patient at Mayo Clinic kept eating the same breakfast - one egg, two slices of whole wheat toast, and a small side of sautéed kale. Her diet didn’t change. She just measured it. Her pharmacist showed her that one cup of kale has 547 µg of vitamin K. One egg? Only 20 µg. Her daily intake was steady at 98 µg. Her INR stayed in range for 11 months straight.
These aren’t outliers. They’re proof. When you make vitamin K intake predictable, your body adapts. Your warfarin dose becomes stable. You stop worrying about every bite.
Tools That Actually Work
Forget apps that just list vitamin K values. You need something that helps you build consistency.
- Use measuring cups - not eyeballing. Research shows visual estimates lead to 45% more variability in intake.
- Track for 4-6 weeks with a food diary. Write down everything you eat that’s green. Not just spinach - broccoli, brussels sprouts, cabbage, even green beans. All count.
- Use a simple template: Breakfast: 1 egg (20 µg), Lunch: ½ cup cooked broccoli (102 µg), Dinner: 3 oz chicken (2 µg). Total: 124 µg. Do this every day. Adjust only if your INR says so.
- Try Warframate - an app with over 2,800 reviews and a 4.7-star rating. It pulls data from USDA FoodData Central and lets you log meals with portion sizes.
Some clinics even use the “Vitamin K Consistency Calculator” - a tool that tells you if your daily intake is within ±15% of your target. That’s the sweet spot. Too much variation? Your INR will drift.
Genetics Matter - But Not Like You Think
Not everyone responds the same way to vitamin K. Some people have a genetic variation in VKORC1 or CYP2C9 that makes them extra sensitive. If you’re one of them, even small changes in your diet can cause big INR shifts.
Studies show these patients may need to keep their vitamin K intake within ±10% variation - not the usual ±20%. That’s tighter. But here’s the good news: you don’t need a genetic test to figure this out. Just monitor your INR closely for the first month. If your numbers jump around even with steady eating, talk to your pharmacist. You might be in that 15-30% of people where diet plays a bigger role.
And yes - about 15-30% of INR swings still can’t be explained. Stress, illness, antibiotics, even changes in alcohol intake can throw things off. But vitamin K? That’s the one you can control.
What to Do When You’re Unsure
Don’t panic. Don’t skip your greens. Don’t start taking vitamin K supplements unless your doctor says so. Here’s what to do instead:
- Find out your target INR range. Is it 2.0-3.0? 2.5-3.5? Know it.
- Identify your usual vitamin K sources. Spinach? Kale? Broccoli? Pick 2-3 and stick with them.
- Measure portions. Use a measuring cup. Not a handful.
- Keep it consistent. Eat the same amount on the same days each week.
- Track your intake for 4-6 weeks. Use a notebook or app.
- Talk to your anticoagulation pharmacist. They’ve seen this a thousand times.
One study found that patients who got counseling from a certified anticoagulation pharmacist had 82% time in therapeutic range - compared to 63% for those who didn’t. That’s not a small difference. That’s life-changing.
What About Supplements?
Some patients are told to take vitamin K supplements to stabilize their INR. That sounds backwards - but it works in some cases.
A landmark study in Blood gave unstable patients 150 µg of vitamin K daily. Their time in range went from 58.4% to 65.6%. No more bleeding. No more clots. Just better control.
But here’s the catch: this only works if you’re already inconsistent. If you’re already eating 80-100 µg daily, adding more won’t help. It might hurt. Supplements aren’t a fix for poor habits. They’re a tool for people who can’t get enough from food - or whose bodies are too sensitive.
Only take them if your pharmacist or doctor recommends it - and never without knowing your exact dose.
Final Rule: Predictable, Not Perfect
You don’t need to be perfect. You don’t need to eat the same exact meal every day. You just need to be predictable.
One week, you eat spinach. Next week, you eat kale. That’s fine - as long as it’s the same amount. One day, you skip greens. That’s okay - as long as you don’t binge on them the next day.
The goal isn’t to avoid vitamin K. It’s to make sure your body knows what to expect. When your diet is steady, your INR is steady. When your INR is steady, you’re safe. And that’s the whole point of being on warfarin.
Can I eat kale every day if I’m on warfarin?
Yes - but only if you eat the same amount every day. One cup of raw kale has 547 µg of vitamin K. If you eat that daily, your body adapts. If you eat it one day and nothing green for three days after, your INR will swing. Consistency matters more than the food itself.
Do I need to avoid green vegetables on warfarin?
No. In fact, avoiding them can make your INR less stable. The current guidelines say vitamin K restriction is harmful. The goal is to eat vitamin K-rich foods regularly and consistently - not to cut them out.
What happens if I eat a lot of vitamin K one day?
Your INR may drop below target, making your blood less thin and increasing your risk of clotting. This can happen within 24-48 hours. If you accidentally eat a large amount of greens, contact your anticoagulation clinic. They may adjust your warfarin dose or schedule an earlier INR test.
Is it safe to take vitamin K supplements while on warfarin?
Only under medical supervision. Some patients benefit from a fixed daily dose (like 150 µg) to stabilize INR, but this must be personalized. Taking supplements without knowing your baseline intake can cause dangerous drops in INR. Never start a supplement without talking to your pharmacist.
How long does it take for dietary changes to affect my INR?
Changes in vitamin K intake can affect your INR within 24-72 hours. That’s why sudden dietary shifts - like a big salad after a week of no greens - can be risky. For this reason, experts recommend tracking your intake for at least 4-6 weeks to find your personal rhythm.
Can antibiotics affect my INR while I’m on warfarin?
Yes. Some antibiotics (like metronidazole and ciprofloxacin) can increase warfarin’s effect, raising your INR and bleeding risk. Others may reduce vitamin K production in your gut, also affecting INR. Always tell your doctor you’re on warfarin before starting any new medication - even over-the-counter ones.
If you’re on warfarin, your diet isn’t the enemy. Inconsistency is. The best thing you can do isn’t to avoid food - it’s to know what you’re eating, measure it, and repeat it. That’s how you stay safe. That’s how you live well.




So let me get this straight - we’re not supposed to avoid kale, but we’re supposed to eat the same amount every Tuesday and Thursday like it’s a damn church service? I love this. Finally, a medical regimen that feels like a cult, but one where the sacrament is a spinach smoothie and the holy text is USDA FoodData Central. Bring on the measuring cups. I’ll bring the wine.
Also, who designed Warframate? A pharmacist with a sense of humor and a grudge against eyeballing? 4.7 stars? That’s not an app - that’s a lifestyle brand.
From a pharmacokinetic standpoint, this is a textbook case of homeostatic disruption via dietary oscillation. The VKORC1 enzyme’s half-life and the hepatic recycling kinetics of vitamin K create a narrow therapeutic window - especially when you introduce non-linear absorption dynamics from raw vs. cooked greens.
What’s fascinating is that the body’s carboxylation efficiency plateaus around 90–110 µg/day. Beyond that, you’re not getting more clotting factors - just noise. The real win isn’t consistency - it’s entropy minimization. Track, don’t guess. Measure, don’t feel. Your INR is a time-series signal. Treat it like one.
This is one of the most thoughtful explanations I’ve read on warfarin management. As someone from India where diets vary wildly between regions - dal and spinach curry one day, rice and lentils the next - the idea of consistency over restriction resonates deeply.
My uncle has been on warfarin for 8 years. He eats one cup of sautéed methi (fenugreek leaves) every Sunday. No more, no less. His INR has been stable since 2018. No hospital visits. No panic. Just routine. It’s not about fear. It’s about rhythm. Thank you for articulating this so clearly.
YESSSS this is the vibe I needed 😭✨ I used to avoid greens like they were radioactive until my pharmacist handed me a measuring cup and said, "Eat this much, every Tuesday. No more, no less." Two months later, my INR was in range 80% of the time. I even started calling my spinach "my little blood thinner baby."
PS: Warframate changed my life. I’m now a certified veggie nerd. 🌿📊 #WarfarinLife #NoMoreGuessing
So… I just eat kale when I feel like it. My INR’s fine. Maybe I’m just lucky. Or maybe all this tracking is just Big Pharma’s way of selling apps. 🤷♀️
There is a profound truth in this: stability is not merely a medical goal - it is a philosophical one. To live with warfarin is to embrace the discipline of repetition, the dignity of routine, and the quiet courage of showing up for your body, day after day.
It is not about control. It is about harmony. Not with food. Not with doctors. But with time. With rhythm. With the quiet pulse of life that does not demand perfection - only presence.
Thank you for this reminder.
Bro this is 100% spot on. I used to freak out every time I ate a salad. Then I found out my usual lunch - 1/2 cup cooked broccoli + 1 egg - was at 122 µg. Same every day. Boom. INR stable for 14 months. No drama. No supplements. Just a measuring cup and a chill attitude.
Also, Warframate is legit. I’ve recommended it to three friends. One of them cried. Not from sadness. From relief.
yo i used to think i had to be some kinda salad monk to stay alive on warfarin but nah
turns out i just needed to stop being a chaotic gremlin with my greens
now i eat 1 cup kale tues/thurs like a robot and my doc says im "a poster child for compliance"
also i call my spinach "the silent bodyguard" 😎
Let me be perfectly clear: this is not just medical advice. This is a revolution in patient autonomy. The fact that we’ve been misled for decades - told to avoid vitamin K, when the real enemy was inconsistency - is a scandal. It’s negligence dressed as caution.
Patients were not educated. They were frightened. And now, thanks to this post, a new standard is emerging - one based on data, not dogma. This is the future of anticoagulation care. And it’s beautiful.
They want you to track your kale like it’s a nuclear reactor because they’re hiding the truth - vitamin K isn’t the problem. It’s the warfarin. It’s outdated. Toxic. A relic from the 1950s. They keep you dependent on blood tests and apps because the real cure - direct oral anticoagulants - is too expensive for them to push.
They don’t care if you eat spinach on Tuesdays. They care if you keep coming back. The system isn’t helping you. It’s monetizing your fear.
Most people on warfarin are dumb. They eat random greens, skip tests, think they know better. This post is smart. But still too soft. You need to track every gram. Every microgram. Every bite. If you miss one day, you reset the whole week. No excuses. No vibes. Just numbers. That’s how you survive.
I’ve spent 12 years as a nurse in an anticoagulation clinic. I’ve seen patients bleed out because they ate a giant salad after a week of no greens. I’ve seen others thrive because they ate the same 90 µg of vitamin K every Tuesday and Thursday - like clockwork.
What this post says is true. But what it doesn’t say is this: the hardest part isn’t the measuring. It’s the mindset. You have to stop seeing food as freedom or restriction. You have to see it as medicine. And medicine doesn’t negotiate. It waits. And it works - if you let it.
Thank you for reminding us what consistency really looks like.